Epidemiological studies have reported strong association between sleep loss and hypertension with unknown mechanisms. This study investigated macrovascular and microcirculation changes and inflammatory markers during repetitive sleep restriction. Sex differences were also explored. Forty-five participants completed a 22-day in-hospital protocol. Participants were assigned to, (1) eight-hour sleep per night (control), or (2) sleep restriction (SR) condition: participants slept from 0300 to 0700 h for three nights followed by a recovery night of 8-h sleep, repeated four times. Macrocirculation assessed by flow mediated dilation (FMD) and microcirculation reactivity tests were performed at baseline, last day of each experimental block and during recovery at the end. Cell adhesion molecules and inflammatory marker levels were measured in blood samples. No duration of deprivation (SR block) by condition interaction effects were found for FMD, microcirculation, norepinephrine, cell adhesion molecules, IL-6 or IL-8. However, when men and women were analyzed separately, there was a statistical trend (p = 0.08) for increased IL-6 across SR blocks in women, but not in men. Interestingly, men showed a significant progressive (dose dependent) increase in skin vasodilatation (p = 0.02). A novel and unexpected finding was that during the recovery period, men that had been exposed to repeated SR blocks had elevated IL-8 and decreased norepinephrine. Macrocirculation, microcirculation, cell adhesion molecules, and markers of inflammation appeared to be resistant to this model of short-term repetitive exposures to the blocks of shortened sleep in healthy sleepers. However, men and women responded differently, with women showing mild inflammatory response and men showing more vascular system sensitivity to the repetitive SR.
Publications
2021
2020
Pain can be both a cause and a consequence of sleep deficiency. This bidirectional relationship between sleep and pain has important implications for clinical management of patients, but also for chronic pain prevention and public health more broadly. The review that follows will provide an overview of the neurobiological evidence of mechanisms thought to be involved in the modulation of pain by sleep deficiency, including the opioid, monoaminergic, orexinergic, immune, melatonin, and endocannabinoid systems; the hypothalamus-pituitary-adrenal axis; and adenosine and nitric oxide signaling. In addition, it will provide a broad overview of pharmacological and non-pharmacological approaches for the management of chronic pain comorbid with sleep disturbances and for the management of postoperative pain, as well as discuss the effects of sleep-disturbing medications on pain amplification.
Recent discoveries demonstrate a critical role for circadian rhythms and sleep in immune system homeostasis. Both innate and adaptive immune responses - ranging from leukocyte mobilization, trafficking, and chemotaxis to cytokine release and T cell differentiation -are mediated in a time of day-dependent manner. The National Institutes of Health (NIH) recently sponsored an interdisciplinary workshop, "Sleep Insufficiency, Circadian Misalignment, and the Immune Response," to highlight new research linking sleep and circadian biology to immune function and to identify areas of high translational potential. This Review summarizes topics discussed and highlights immediate opportunities for delineating clinically relevant connections among biological rhythms, sleep, and immune regulation.
2019
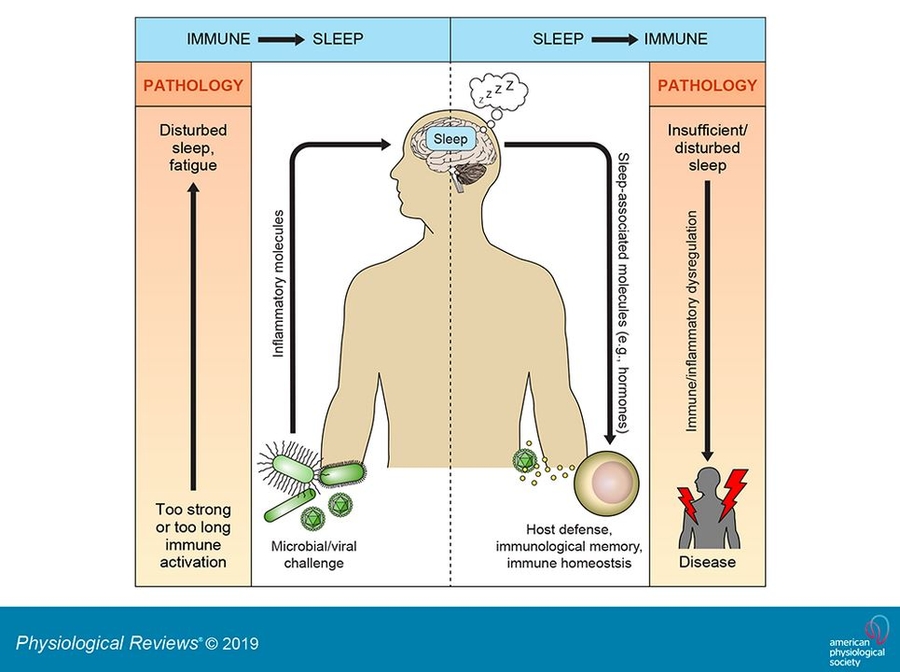
Sleep and immunity are bidirectionally linked. Immune system activation alters sleep, and sleep in turn affects the innate and adaptive arm of our body's defense system. Stimulation of the immune system by microbial challenges triggers an inflammatory response, which, depending on its magnitude and time course, can induce an increase in sleep duration and intensity, but also a disruption of sleep. Enhancement of sleep during an infection is assumed to feedback to the immune system to promote host defense. Indeed, sleep affects various immune parameters, is associated with a reduced infection risk, and can improve infection outcome and vaccination responses. The induction of a hormonal constellation that supports immune functions is one likely mechanism underlying the immune-supporting effects of sleep. In the absence of an infectious challenge, sleep appears to promote inflammatory homeostasis through effects on several inflammatory mediators, such as cytokines. This notion is supported by findings that prolonged sleep deficiency (e.g., short sleep duration, sleep disturbance) can lead to chronic, systemic low-grade inflammation and is associated with various diseases that have an inflammatory component, like diabetes, atherosclerosis, and neurodegeneration. Here, we review available data on this regulatory sleep-immune crosstalk, point out methodological challenges, and suggest questions open for future research.
Despite known associations of insomnia disorder with alterations in cytokine and glucocorticoid (GC) production, neither the sensitivity of immune cells to a GC signal nor the reactivity of the hypothalamus-pituitary-adrenal (HPA) axis and inflammatory system to stress, or adaptation of these systems to repeated stress have been assessed in patients with insomnia. To investigate potential dysregulation in stress reactivity and adaptation to repeated exposure, a physiological stressor (the cold pressor test; CPT) was repeatedly administered to N = 20 participants with insomnia disorder (based on DSM-V, 18 females, age 30 ± 2.5 years) and N = 20 sex-matched healthy controls following an at-home actigraphy and in-laboratory PSG. HPA and inflammatory markers (serum cortisol, plasma interleukin [IL]-6) were measured at baseline/resting levels and following each of the three CPTs. In addition, sensitivity of monocytes to the synthetic GC dexamethasone was assessed in-vitro at baseline levels in order to examine the cortisol-IL-6 interplay at the cell level. Compared to healthy controls, individuals with insomnia disorder exhibited shorter sleep duration as assessed by actigraphy and PSG (p ≤ 0.05). HPA, but not inflammatory reactivity to the repeated CPT challenge was greater in insomnia disorder (p ≤ 0.05 for group effect), due to greater cortisol responses to the initial CPT (p ≤ 0.05). There were no between-group differences in the ability of the HPA to adapt to stress repetition nor in basal/resting levels of cortisol, IL-6, and GC sensitivity. These findings suggest that insomnia disorder potentiates HPA axis reactivity to initial/novel stressors, which may constitute a pathway underlying adverse health consequences in the long term.

While it is well established that slow-wave sleep electroencephalography (EEG) rebounds following sleep deprivation, very little research has investigated autonomic nervous system recovery. We examined heart rate variability (HRV) and cardiovagal baroreflex sensitivity (BRS) during four blocks of repetitive sleep restriction and sequential nights of recovery sleep. Twenty-one healthy participants completed the 22-day in-hospital protocol. Following three nights of 8-hr sleep, they were assigned to a repetitive sleep restriction condition. Participants had two additional 8-hr recovery sleep periods at the end of the protocol. Sleep EEG, HRV, and BRS were compared for the baseline, the four blocks of sleep restriction, and the second (R2) and third (R3) nocturnal recovery sleep periods following the last sleep restriction block. Within the first hour of each sleep period, vagal activation, as indexed by increase in high frequency (HF; HRV spectrum analysis), showed a rapid increase, reaching its 24-hr peak. HF was more pronounced (rebound) in R2 than during baseline (p < 0.001). The BRS increased within the first hour of sleep and was higher across all sleep restriction blocks and recovery nights (p = 0.039). Rebound rapid eye movement sleep was observed during both R2 and R3 (p = 0.004), whereas slow-wave sleep did not differ between baseline and recovery nights (p > 0.05). Our results indicate that the restoration of autonomic homeostasis requires a time course that includes at least three nights, following an exposure to multiple nights of sleep curtailed to about half the normal nightly amount.
BACKGROUND: Fibromyalgia (FM) is a chronic widespread pain disorder characterized by negative affect, sleep disturbance, and fatigue. This uncontrolled pilot study investigated the efficacy of daily yoga-based exercise to improve FM symptoms and explored baseline phenotypic characteristics associated with the greatest benefit.
METHODS: FM patients (n=46, with 36 completers) reported psychosocial functioning and a range of FM symptoms using validated instruments before and after participation in Satyananda yoga, which included weekly in-person pain-tailored group classes for 6 weeks and daily home yoga video practice.
RESULTS: Changes in FM symptoms from pre- to post-yoga were variable amongst participants. Group means for pain decreased, as reported by average daily diary and Brief Pain Inventory, with greater home practice minutes associated with a greater decrease in pain. Average daily ratings of sleep and fatigue improved. Pain catastrophizing was decreased overall, with greater change correlated to a decrease in FM symptoms. We did not observe any group mean changes in actigraphy sleep efficiency, Patient-Reported Outcomes Measurement Information System-anxiety and the Revised Fibromyalgia Impact Questionnaire. Multilevel Modeling analysis revealed a significant interaction between anxiety and catastrophizing for end-study sleep efficiency, fatigue, and pain, such that patients with higher baseline catastrophizing and lower baseline anxiety reported less pain and fatigue, and higher sleep efficiency after the sixth week of yoga practice.
CONCLUSION: This pilot study suggests that yoga may reduce pain and catastrophizing, as well as improve sleep, but these changes were modest across study participants. Greater uptake of home yoga practice as well as a phenotype of higher baseline catastrophizing combined with lower baseline anxiety were associated with greater impact. Future randomized, controlled trials comparing different types of yoga or exercise will allow determination of the most effective treatments for FM and allow closer targeting to the patients who will benefit most from them.
While it is well established that slow-wave sleep electroencephalography (EEG) rebounds following sleep deprivation, very little research has investigated autonomic nervous system recovery. We examined heart rate variability (HRV) and cardiovagal baroreflex sensitivity (BRS) during four blocks of repetitive sleep restriction and sequential nights of recovery sleep. Twenty-one healthy participants completed the 22-day in-hospital protocol. Following three nights of 8-hr sleep, they were assigned to a repetitive sleep restriction condition. Participants had two additional 8-hr recovery sleep periods at the end of the protocol. Sleep EEG, HRV, and BRS were compared for the baseline, the four blocks of sleep restriction, and the second (R2) and third (R3) nocturnal recovery sleep periods following the last sleep restriction block. Within the first hour of each sleep period, vagal activation, as indexed by increase in high frequency (HF; HRV spectrum analysis), showed a rapid increase, reaching its 24-hr peak. HF was more pronounced (rebound) in R2 than during baseline (p < 0.001). The BRS increased within the first hour of sleep and was higher across all sleep restriction blocks and recovery nights (p = 0.039). Rebound rapid eye movement sleep was observed during both R2 and R3 (p = 0.004), whereas slow-wave sleep did not differ between baseline and recovery nights (p > 0.05). Our results indicate that the restoration of autonomic homeostasis requires a time course that includes at least three nights, following an exposure to multiple nights of sleep curtailed to about half the normal nightly amount.
2018
Chronic pain conditions are highly comorbid with insufficient sleep. While the mechanistic relationships between the 2 are not understood, chronic insufficient sleep may be 1 pathway through which central pain-modulatory circuits deteriorate, thereby contributing to chronic pain vulnerability over time. To test this hypothesis, an in-laboratory model of 3 weeks of restricted sleep with limited recovery (5 nights of 4-hour sleep per night followed by 2 nights of 8-hour sleep per night) was compared with 3 weeks of 8-hour sleep per night (control protocol). Seventeen healthy adults participated, with 14 completing both 3-week protocols. Measures of spontaneous pain, heat-pain thresholds, cold-pain tolerance (measuring habituation to cold over several weeks), and temporal summation of pain (examining the slope of pain ratings during cold water immersion) were assessed at multiple points during each protocol. Compared with the control protocol, participants in the sleep-restriction protocol experienced mild increases in spontaneous pain (P < 0.05). Heat-pain thresholds decreased after the first week of sleep restriction (P < 0.05) but normalized with longer exposure to sleep restriction. By contrast, chronic exposure to restricted sleep was associated with decreased habituation to, and increased temporal summation in response to cold pain (both P < 0.05), although only in the past 2 weeks of the sleep-restriction protocol. These changes may reflect abnormalities in central pain-modulatory processes. Limited recovery sleep did not completely resolve these alterations in pain-modulatory processes, indicating that more extensive recovery sleep is required. Results suggest that exposure to chronic insufficient sleep may increase vulnerability to chronic pain by altering processes of pain habituation and sensitization.
Chronic sleep restriction and obesity are two major public health concerns. This study investigated how chronic sleep restriction changes implicit attitudes towards low- and high-calorie foods. In a randomized, counterbalanced cross-over design, 17 participants (eight females, nine males) underwent two laboratory testing sessions where they were either sleep-restricted for 3 weeks (i.e. underwent three weekly cycles of 5 nights of 4 h of sleep followed by 2 nights of 8 h of sleep opportunity) or received 3 weeks of control sleep (i.e. 8 h of sleep opportunity per night for 3 weeks). There was evidence for a significant sleep condition x sex interaction (F(1, 20) = 4.60, P = 0.04). After chronic sleep restriction, men showed a trend towards a significant decrease in their implicit attitudes favouring low-calorie foods (P = 0.08), whereas women did not show a significant change (P = 0.16). Men may be at increased risk of weight gain when sleep-deprived due to a reduced bias towards low-calorie foods.