Research
Research Areas
Delineating HFpEF risk and scope:
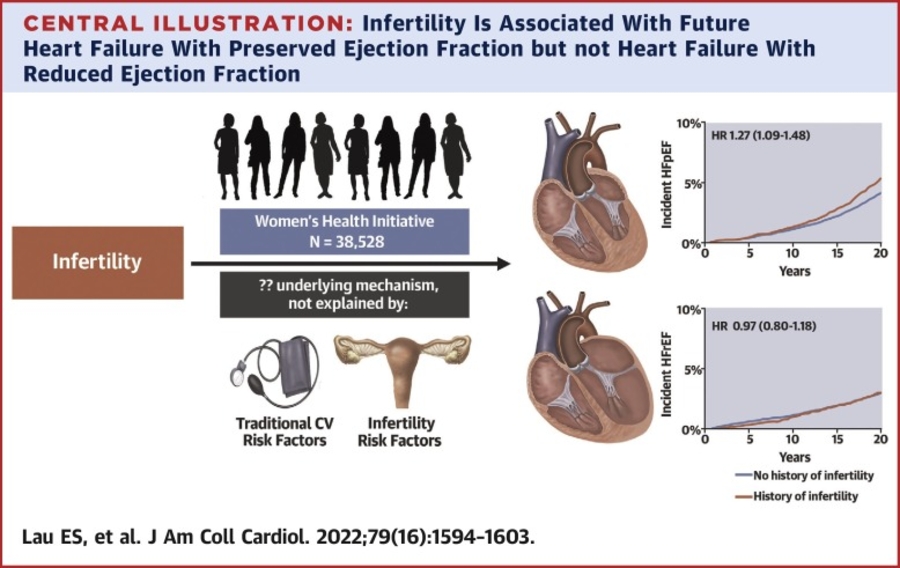
We have collaborated with multiple community-based epidemologic cohorts with >22,000 individuals followed prospectively for incident HF, which has enabled seminal insights stemming from this effort. For example, we demonstrated that clinical precursors of HFpEF vs HFrEF are distinct, and that traditional clinical risk models and cardiovascular biomarkers predict HFpEF less well than HFrEF, underscoring the need for better molecular phenotyping. Importantly, we showed that obesity and cardiometabolic factors including insulin resistance are central determinants of future HFpEF. We have highlighted important sex differences in HFpEF, including female-specific risk enhancers such as infertility. Recent work is focused on machine-learning approaches to refine our epidemiologic understanding of HFpEF, through the Broad Institute’s Machine Learning for Health initiative.
HFpEF molecular mechanisms of disease:
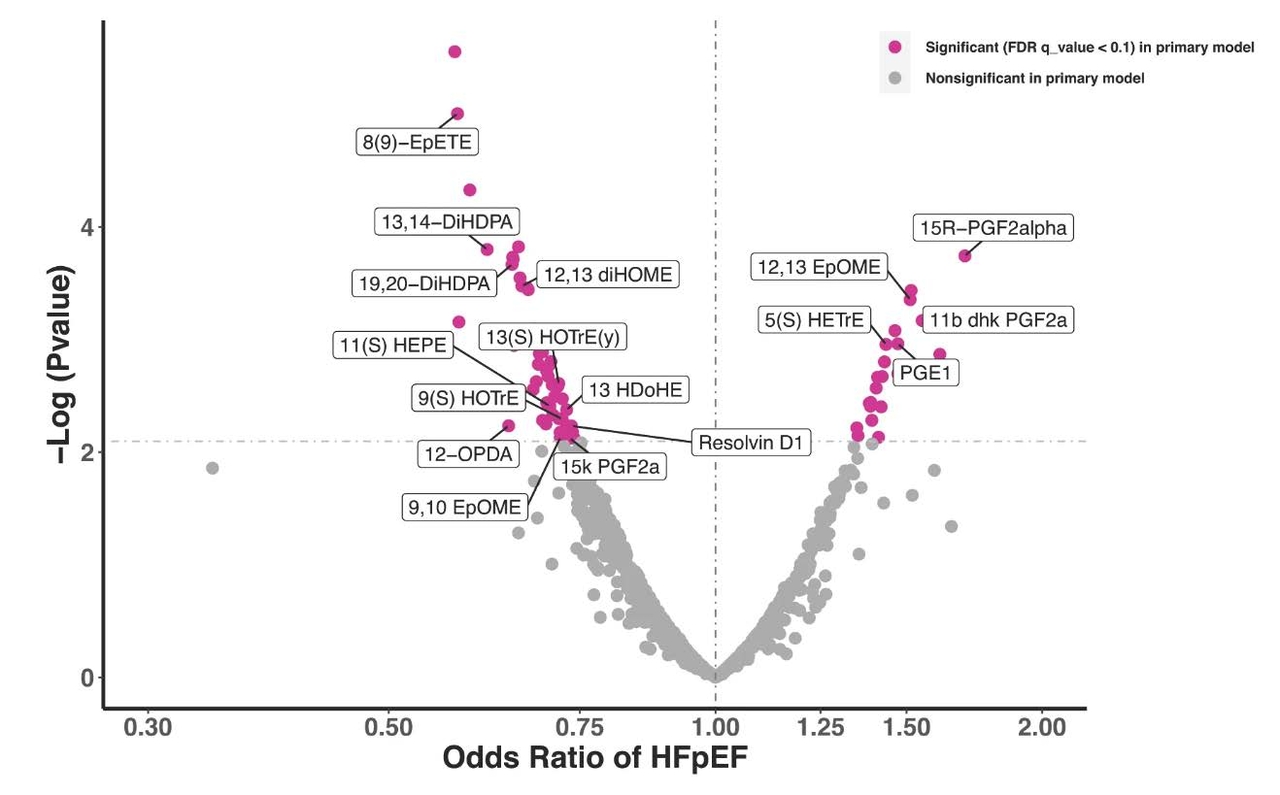
Our laboratory has leveraged molecular profiling to examine proteomic and metabolic signatures of HFpEF, work that established systemic inflammation and adiposity-related pathways as a central contributor to HFpEF development. Our group has demonstrated that eicosanoid and novel related bioactive lipids, known to govern upstream initiation of pro- and anti-inflammatory activity, are associated with HFpEF. Specifically, prostaglandin and linoleic acid derivatives are associated with greater odds, and epoxides and oxlipins with lower odds of HFpEF.
Inter-organ communication in HFpEF:
An important focus of the laboratory has been to understand cardiac-vascular and cardiac-pulmonary interactions as important contributors to HFpEF pathophysiology. We previously demonstrated enhanced large artery stiffness as an important determinant of diastolic reserve. We currently are using novel approaches to isolate human venous endothelial cells to better understand the interaction between endothelial health, cardiometabolic disease, and HFpEF.
