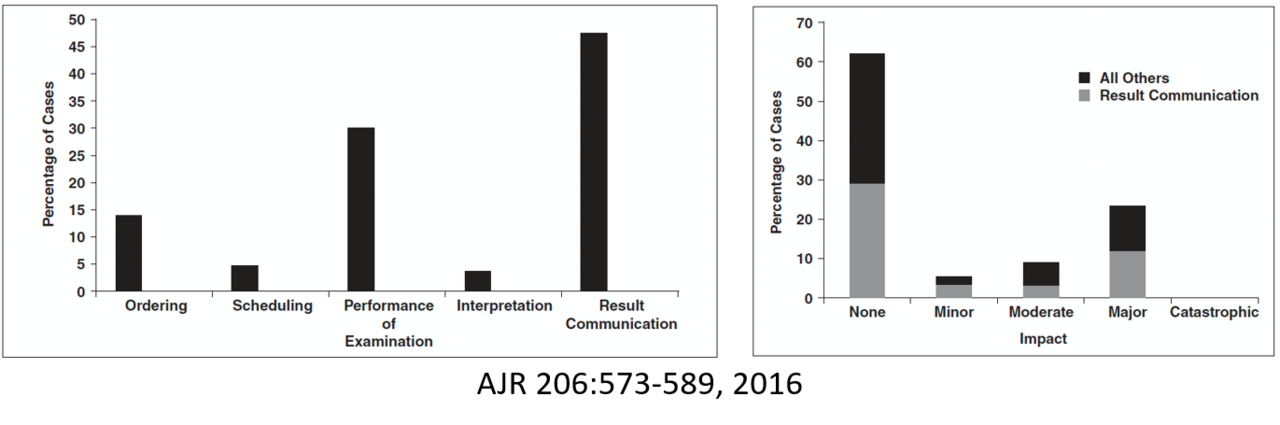
Communication errors: We sought to analyze the types of communication errors in radiology, investigate at which step communication errors occur, and evaluate the impact of communication errors on patient care, customer satisfaction, and workflow efficiency to identify opportunities for quality improvement.
While errors in communication during result communication to referring physicians might be an expected source of errors, we found that about 50% of communication errors occurred during other aspects of the radiology process, including ordering, scheduling, performance of examination, and interpretation. These resulted in a range of impacts on patient care.
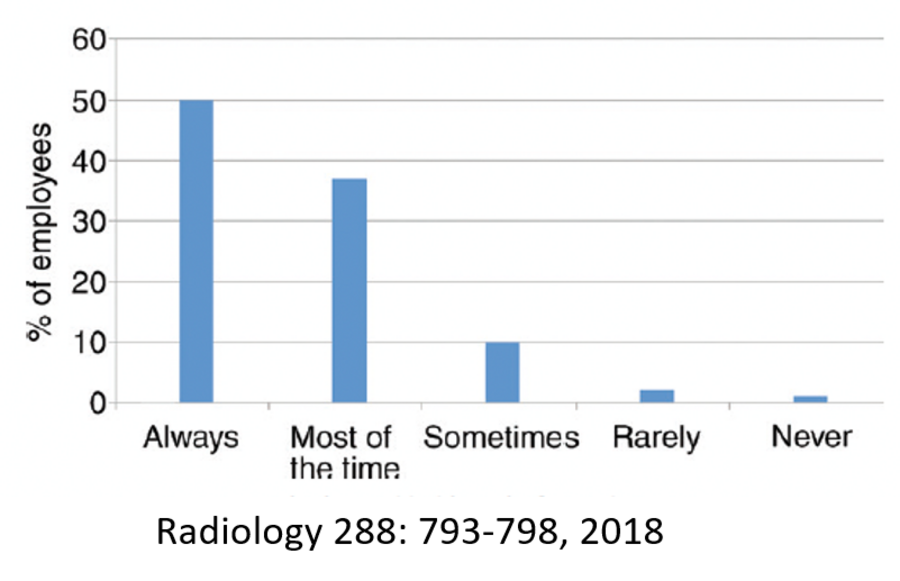
Speaking up to identify safety issues: Implementing safety improvements requires reporting of safety events. In a study of employees in our department, we found that 50% of employees spoke up less than 100% of the time. The most commonly reported barriers to speaking up included a high reporting threshold, reluctance to challenge authority, fear of disrespect, and lack of listening.
Implementing solutions: Most importantly, identifying the barriers to reporting safety events enables the implementation of countermeasures to improve safety.
Countermeasures to identified barriers are shown here:
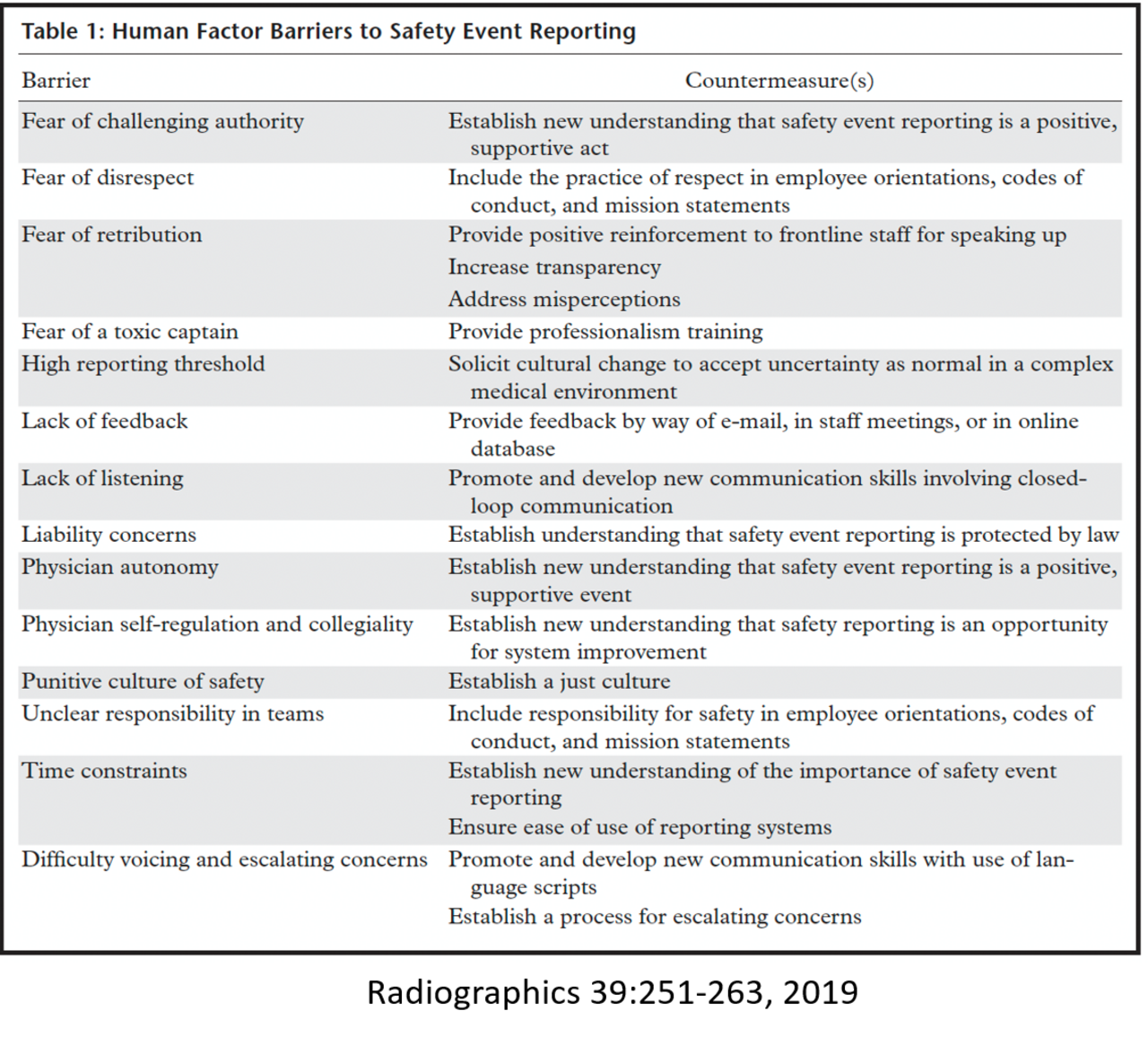
Together, these studies identified multiple areas for improvement within the department and helped to create a climate of openness and a community working towards improvement.