Deep brain stimulation (DBS) of the ventral intermediate (VIM) nucleus of the thalamus is an approved treatment for essential tremor, and is typically performed using intraoperative neurophysiologic confirmation, requiring the patient to remain awake throughout the surgery. Recently, DBS placement under general anesthesia has become an alternative for targets in Parkinson’s Disease patients. Extending this asleep method to targeting the VIM for essential tremor has been limited due to difficulty visualizing the relevant anatomical brain target. The use of tractography can augment visualization of the DBS target.
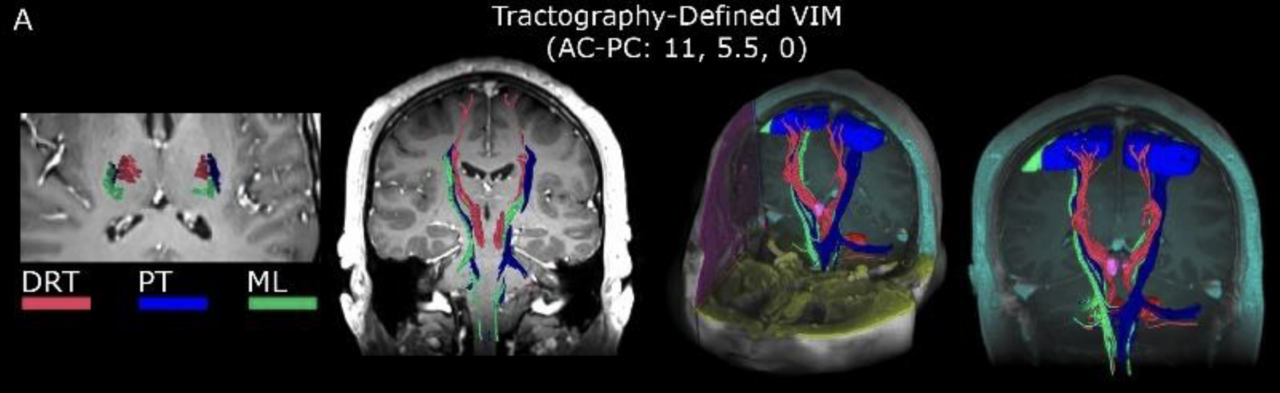
MRI tractography can be used to visualize key structures such as the dentato-rubro-thalamic tract (DRT) as well as "avoid" regions such as the medial lemniscus (ML) and pyramidal tract (PT). At BIDMC this has become our standard targeting protocol for asleep VIM placement.
In this study, we are retrospectively reviewing VIM DBS surgeries using this asleep protocol and comparing them with cases previously done using traditional awake micro electrode recordings. We are modeling the volume of tissue activated based on the DBS implant and clinical settings and evaluating whether the degree of activation of the DRT correlates with clinical outcome.