What is Deep Brain Stimulation?
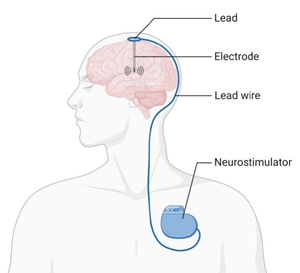
Deep brain stimulation (DBS) uses leads with electrodes (wires) that are placed in regions of your brain that are specific to your diagnosis. The leads deliver electrical impulses in the designated area of your brain to help alleviate symptoms.
These electrodes connect to a small pacemaker-like device called an Implanted Pulse Generator (IPG). This device is placed in the chest below your collar bone. DBS is adjustable, individualized, can be placed bilaterally (on both sides of your brain) and reversible.
Who benefits from DBS?
Patients who may benefit from DBS surgery include those with Parkinson’s Disease (PD), Dystonia, Essential tremor, Epilepsy, and obsessive-compulsive disorder.
For patients with Parkinson’s Disease:
- DBS improves tremor, stiffness (rigidity), bradykinesia and dyskinesia
- DBS does not eliminate these symptoms completely
- DBS can achieve improvement in symptoms similar to your best response to medication
- DBS is an option if you have Parkinson's tremor that does not respond to medication
- DBS may also be an option if you benefit from medication, but experience medication side effects, motor complications, or significant off times
- You MAY be able to reduce your medication, but do not expect it to stop completely
What kind of DBS devices do we use?
We use the latest advanced DBS devices available from all three companies that make DBS devices, Medtronic, Abbott, and Boston Scientific. All devices available include non-rechargeable and rechargeable options and are effective at treating Parkinson's Disease symptoms. We have summarized some of the differences below.
Medtronic
- Medtronic has segmented Sensight leads that allow for a more precise direct stimulation which can limit side effects
- • The Medtronic Percept IPG can read brain activity from the implanted leads and this information can guide programming and setting adjustments
- This device allows for you to have a full body 3T MRI
- Rechargeable and non-rechargeable IPGs are available. Rechargeable devices are charged wirelessly through the skin for about 30 minutes per week and last over 15 years. Non-rechargeable devices are expected to last for 4-6 years before needing replacement in a minor surgical procedure.
Abbott
- Abbott uses segmented directional leads that allow for direction of stimulation to focus on areas that are important for treatment and can limit side effects.
- The device is able to be programmed for full body 1.5T MRI.
- Abbott has a virtual clinic programming option that allows your neurologist to program your device remotely just as if you were in person.
- Rechargeable and non-rechargeable IPGs are also available.
Prior to Surgery
First you will meet with Dr. Aronson at the Beth Israel Deaconess Neurosurgery Clinic to determine if you are a good candidate for this device.
NEXT STEPS
Several tests may be ordered as part of the workup to determine if you are a surgical candidate:
- MRI – a specific surgical planning MRI may be needed, so this may need to be done even if you have had a previous MRI
- Neuropsychological testing – standard test that is done to evaluate memory and cognition
- On/off testing – standard testing done to evaluate the effectiveness of medications as well as neurological and motor responses.
Once these tests are completed, the results will be reviewed by Dr. Aronson, and you will meet with him again to discuss if you are a good candidate for this surgery.
If you have any concerns at any point, please let Dr. Aronson know. You can also speak with a member of his team in
neurosurgery. It is important to address your concerns at your clinic visit so other needed consults and tests can be arranged, if needed.
SCHEDULING SURGERY
Our office will reach out to you to schedule your surgery, along with sending you a pre-surgical letter with information about the day of your surgery. A nurse from preadmission testing will call you a few days prior to surgery to confirm your surgery date, time, and provide you with parking instructions along with an arrival time.
- Please alert the nurse if you are on any diabetic medications, blood thinners, or medications to treat a substance use disorder.
PREPARING FOR SURGERY
- You should stop taking aspirin and NSAIDs (Motrin, Ibuprofen, Advil, or Aleve) one week prior to surgery.
- If you are taking any blood thinning medications like Plavix, Coumadin (Warfarin), Eliquis (Apixaban), Xarelto, ticagrelor (Brilinta) you will need to contact either your cardiologist or your primary care provider for surgery clearance and instructions on how to stop these medications for surgery.
- The night before surgery do not eat or drink past midnight.
- You may have a small sip of water in the morning with your pills you have been instructed to take the morning of surgery.
- Please bring all of your medications in original pharmacy bottles (not in a pill organizer) with you to the hospital.
- You should continue taking all Parkinson’s disease medications as you usually do.
Day of Surgery
We recommend parking in the Lowry Building Garage, 110 Francis Street, Boston, MA 02215 across from the Klarman Building.

At your assigned arrival time go to the Klarman Building 111 Francis Street, Boston, MA 02215 on the 5th floor to check in at the front desk. You will be brought to the pre-operative area where you will change to a hospital gown. You will meet the anesthesia team and an IV will be placed. You will be taken to the operating room on a stretcher.
You will be asked to remove:
- All jewelry except your wedding band
- Dentures or partials
- Hearing aids
- Contact lenses and eyeglasses
- Hair pieces
- Cosmetics and nail polish (typically remove the night before)
In the Operating Room
DBS surgery has historically been performed with patients awake. With advances in imaging and technology this is no longer necessary. DBS can be performed safely and effectively with patients completely asleep under general anesthesia. Dr. Aronson has performed all DBS surgeries under general anesthesia for nearly 10 years with excellent results.
During surgery you will be completely sedated under general anesthesia. Once you are asleep Dr. Aronson will perform the surgery with both the leads and the generator placed on the same day typically. You will have a CT scan or MRI performed in the operating room to confirm placement of the leads. Surgery takes approximately 4 hours.
After surgery you will be awakened from anesthesia in the operating room and then taken to the recovery room, known as the Post-Anesthesia Care Unit (PACU).
As you are recovering, Dr. Aronson will speak with your family and friends and let them know that your surgery is finished and how things went. Plan to spend one night in the hospital following surgery.
In the Hospital After Surgery
You may experience a slight change in your cognition up to the first week after the electrodes are placed. This is sometimes noticed by others and involves being a little more forgetful.
You may have a transition phase due to lesioning effect in which your symptoms will be better temporarily. This can last an hour or up to a day. Please note that stimulation has not yet been turned on, and original symptoms will return, and sometimes can be slightly worse temporarily.
Plans to go home
A nursing case manager will meet with you prior to discharge to set up any care you may need while at home. Depending on your needs, they may arrange for a visiting nurse, a home health aide, or a physical or occupational therapist.
You may be given a DBS programmer to take home with you. Occasionally this is delivered to your neurologist, who will give it to you at the programming appointment. You may be instructed to use the programmer to log times when you have certain symptoms prior to your first programming appointment but this is not required. Please ensure you bring the programmer with you to the programming appointment with your neurologist. If you have a rechargeable IPG you will also be given the charging system and will receive instructions on how to use it.
After Surgery
Managing the surgery sites
Typically, all incisions are closed with absorbable suture, so the stitches do not need to be removed. They are covered in skin glue. The glue will turn a dark color and eventually flake off. Try not to scratch at or pick off the glue. If a dressing is placed over the chest incision it can be removed the day following surgery.
Managing pain
You may be sent home with a prescription for pain medication or nausea medication if needed. However, most patients find Tylenol (acetaminophen) is sufficient to control any pain. Typically, NSAIDs such as ibuprofen (Motrin, Advil) may be taken starting a week after surgery, unless directed otherwise. If you take a blood thinner instructions will be provided on when and how to resume taking these medications.
What to expect and how you may feel after surgery
You will have some numbness or itching around the incision that can last several weeks after your surgery. Discomfort is usually mild, but you may take extra strength Tylenol to alleviate this.
You will need someone to stay with you to help you with your care for up to the first 48 hours after you get home from your surgery.
Tips, and things to keep in mind for when you are at home
- It is normal to feel tired and have a lack of energy after surgery. Your energy levels will return to normal gradually as your body heals from surgery.
- Pace your activities and rest when needed.
- Avoid vigorous activities, and strenuous exercise for the first four weeks after surgery.
- Avoid lifting anything greater than 10 pounds for the first few weeks after surgery.
- You may shower two days after your surgery allowing water to run over your incisions and patting them dry with a clean towel.
- DO NOT submerge your incision underwater in a bathtub or a pool for up to 6 weeks.
- DO NOT apply lotions or oils to your incision
- Typically, your sutures will be dissolvable and will not need to be taken out. If you have a question about your sutures please call our office.
When to Call Our Office
Beth Israel Deaconess Neurosurgery Office 617-632-7246
- If you experience any unusual swelling, any new numbness, tingling, weakness, or visual changes
- Fever above 101° lasting longer than 24 hours
- Experience any redness, swelling, heat, or drainage from your incision
- If you experience pain that is not relieved by either Tylenol or prescribed pain medication, or if you have trouble re-establishing bowel habits after trying over the counter stool softeners.
Programming your Device After Surgery
Your device will be turned on two weeks after surgery at your neurologist's office. If you have any questions about coordinating the programming visit, please contact Dr. Aronson’s office. The device will be programmed using a computer tablet to adjust the settings of your electrodes.
The initial visit to turn on your device and program it will take one hour, which will involve testing the individual electrodes for benefit and side effects. Your initial device settings will be low, and you may not feel a difference in your symptoms right away
If you were given a programmer to take home with you after surgery, bring it to this appointment. If you were not given the programmer at surgery, it will be given to you at this appointment. You can use the programmer to turn your stimulation on, off, and change settings.
Either our office or the device company will show you how to put your device in MRI or Surgery mode.
You will also need to follow up with Dr. Aronson’s office 4-6 weeks after surgery. This may be arranged as an in-person or telehealth visit.
Negative Side Effects
For the first 3 days after your device has been turned on, we advise not changing the settings, unless you have negative side effects like uncontrolled movements or difficulty walking. The following are general guidelines only; you should discuss management of the DBS settings with your neurologist who is programming the device.
- If you experience any negative side effects, you can decrease the amplitude until the side effects go away and leave the setting there for 3 days.
- If you have significant Parkinson's Disease symptoms you may increase the amplitude by 0.3. If you continue to have symptoms in another 3-5 days, you can increase again by 0.3 and continue to do so until your symptoms improve, or you have met your maximum increase threshold. If symptoms worsen with any increase in DBS return to the lower setting and contact your neurologist.
- DO NOT make changes more than once every 3 days
What to Expect at One Month and Beyond
You will be evaluated by Dr. Aronson in 4-6 weeks in the office or via telehealth.
To obtain the best control of your symptoms you may be required to see your neurologist for several appointments so adjustments can be made. These adjustments must be made slowly so this process may take several months.
For PD patients, the goal is to try and find a balance between a reduction in medication and stimulation to have the best effect on your symptoms.
Please do not make adjustments to your medications on your own. Speak to your neurologist about any changes to medications and dosing.
Your DBS battery will need to be replaced after several years, which will require a small and quick surgical procedure to replace the battery. This will be coordinated with your neurology and neurosurgery team close to the replacement date.
Some patients are implanted with rechargeable IPG devices. These devices need to be recharged regularly and will eventually need replacement, typically around 15 years.